Want to know more about MPS II Hunter? Watch our animated guide.
On this page you can find our animated guide, general information about the condition, latest news, updates and stories and a list of relevant resources and events.
Understanding the condition
What is MPS II?
MPS II, known as Hunter disease, is one of the mucopolysaccharide storage diseases. MPS II was first identified by Dr Hunter in 1917 and includes a spectrum of symptoms from mild to severe.
Mucopolysaccharides are long chains of sugar molecules used in the building of bones, cartilage, skin, tendons and many other tissues in the body. In the course of normal life there is a continuous recycling process of building new mucopolysaccharides and breaking down old ones, which requires special biochemical tools called enzymes.
People with MPS II are missing or are low in an enzyme called iduronate 2-sulphatase, which is essential in breaking down mucopolysaccharides dermatan sulphate and heparan sulphate.
When dermatan sulphate and heparan sulphate are not completely broken down they remain stored in the body, and this causes the symptoms that people with MPS II experience.
Oliver and Sam
Oliver and Sam have Hunter disease because their bodies are missing a special enzyme. It makes their skin cells clog up, causes stiffness of their joints and makes it harder to breathe.

Frequently asked questions
Mucopolysaccharides are long chains of sugar molecules used in the building of bones, cartilage, skin, tendons and many other tissues in the body. “Muco” refers to the thick jelly-like consistency of the sugar molecules, “poly” means many, and “saccharide” is a general term for the sugar part of the molecule. In the course of normal life there is a continuous recycling process of building new mucopolysaccharides and breaking down old ones. The breakdown and recycling process requires a series of special biochemical tools called enzymes.
People with MPS II are missing or are low in an enzyme called iduronate 2-sulphatase, which is essential in breaking down mucopolysaccharides dermatan sulphate and heparan sulphate. When dermatan sulphate and heparan sulphate are not completely broken down they remain stored in the body. The symptoms of MPS II are a result of the build-up of dermatan sulphate and heparan sulphate in the tissues in the body. Babies may show little sign of the disease but as more and more cells build up with partially broken down mucopolysaccharides, symptoms start to appear.
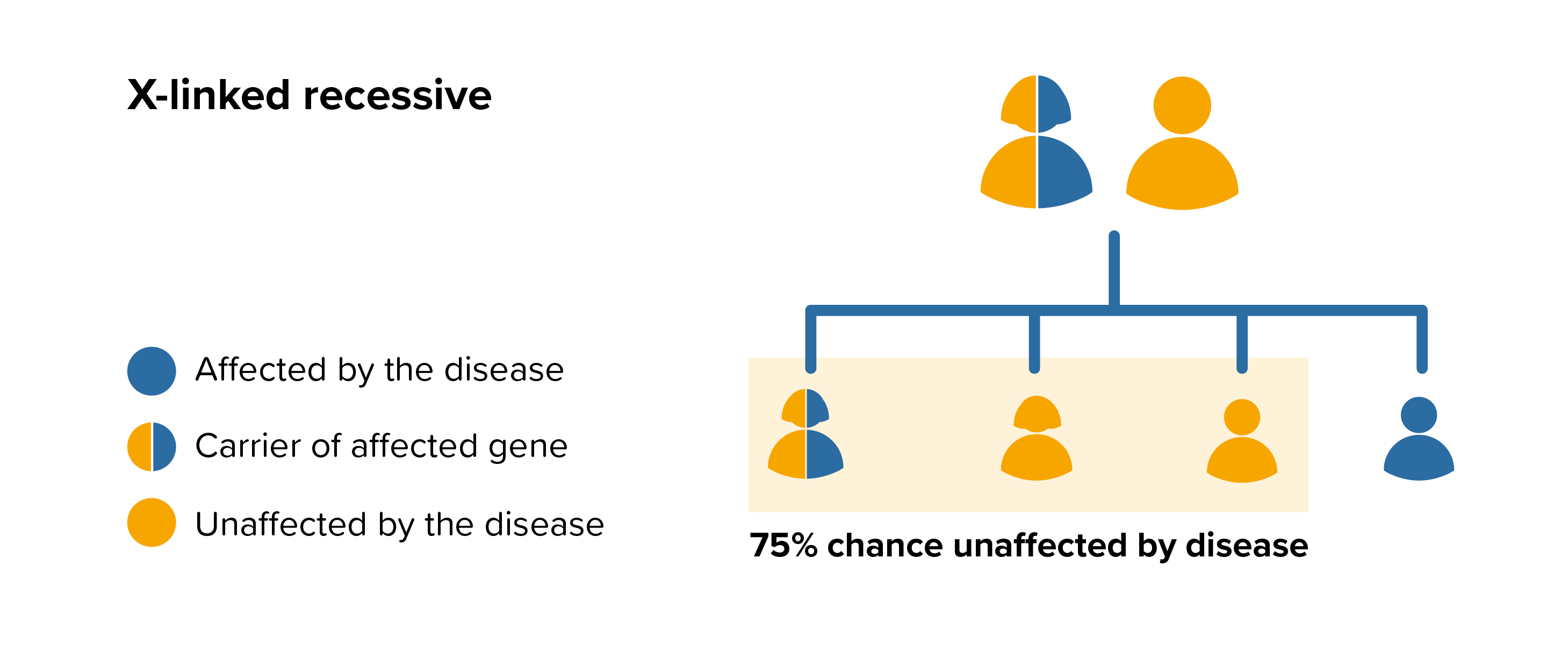
MPS II is an X-linked recessive disease this means that the female are carriers of the affected gene and, apart from very rare cases, only males will be affected by MPS II. It is different for other MPS diseases which are autosomal recessive diseases this means that both parents must carry the same affected gene, and each pass this same affected gene to their child.
People probably carry from 5 to 10 genes with mutations in each of their cells. Problems happen when the particular gene is dominant or when a mutation is present in both copies of a recessive gene pair. Genes are the unique set of instructions inside our bodies that make each of us an individual. They are the blueprint for our growth and development, as well as controlling how our bodies function.
Genes are carried on structures called chromosomes and it is usual to have 23 pairs. A child will inherit half of the chromosomes from the mother and the other half from the father resulting in 23 pairs. 22 of these pairs look the same in both males and females. Pair 23 are the sex chromosomes, and this is the pair that differ between females and males. The X chromosome is inherited from the mother and the Y chromosome is inherited from the father. More information about inheritance is available in our guide to inheritance.
For each pregnancy the chances of a baby inheriting MPS II are completely independent of whether a previous child was affected with MPS II. For a female carrier of MPS II there is a 50% (1:2) risk that any male born to her will have the disease. Furthermore, there is a 50% (1:2) risk that any female born to her will be a carrier for the disease. The sisters and maternal aunts of a male with MPS II may be carriers of the disease and would also have the same risk of passing the affected gene to any male born to them.
 All parents of children with MPS II can benefit from genetic counselling, the counsellor can provide advice on the risk to close relatives and to suggest whether the wider family should be informed. To find out during a pregnancy, if the baby is affected by MPS II, screening tests can be arranged early on during a pregnancy for those families who already have a child with MPS II. Carrier screening is an option for females but it is not 100% reliable or accurate and is not possible in all cases. Amniocentesis and chorionic villus sampling are both available during the pregnancy to find out if the baby is affected by MPS II.
All parents of children with MPS II can benefit from genetic counselling, the counsellor can provide advice on the risk to close relatives and to suggest whether the wider family should be informed. To find out during a pregnancy, if the baby is affected by MPS II, screening tests can be arranged early on during a pregnancy for those families who already have a child with MPS II. Carrier screening is an option for females but it is not 100% reliable or accurate and is not possible in all cases. Amniocentesis and chorionic villus sampling are both available during the pregnancy to find out if the baby is affected by MPS II.
It might also be possible to have Pre-implantation genetic diagnosis (PGD) screening to avoid passing MPS II to the baby. PGD is an assisted fertility treatment that involves checking the chromosomes of embryos before they are transferred in the womb using IVF techniques.
It is estimated that nearly 6% of the UK population (around 3.5million people) will be affected by a rare disease at some point in their lives. A single rare disease may affect up to about 30,000 people however the vast majority of rare diseases affect far fewer than this.
During a 10 year period (1992 to 2002) 52 babies were born with MPS II the UK.
People with MPS II can experience some or many symptoms from a wide spectrum which range from severe to very mild. Historically MPS II had been described as either mild or severe, however based on current understanding of the enzyme and its gene, MPS II comprises a wide spectrum of symptoms and severity.
Some people with MPS II will have progressive developmental delay and severe progressive physical problems. Others will have normal intelligence and progressive physical problems, some being more severely affected than others.
It is important to remember that MPS II is extremely varied in its effects and may even vary in its effects between siblings and generations.
For more on the symptoms, see:
Enzyme Replacement Therapy (ERT)
For people with MPS II ERT is a long-term therapy whereby the missing or deficient enzyme is given via an intravenous infusion. The name for the replacement enzyme in MPS II is idursulfase and the brand name is Elaprase®. Elaprase® was licensed as an ERT in 2007 and has been shown to reduce many of the non-brain related symptoms, such as improving respiratory function and mobility and reducing joint stiffness.
Elaprase ® is a weekly infusion lasting between 1 to 3 hours that can be administered at home. More information about Elaprase ® can be found at www.elaprase.com and a UK version of the patient information leaflet is here. Further information on this treatment is available from the electronic medicines compendium.
For an up-to-date list of current UK based trials taking place visit Be Part of Research (resource provided by the National Institute for Health Research). For an international search visit Clinical Trials (resource provided by the U.S. National Library of Medicine).
This resource provides information on trial status including recruiting, completed or withdrawn and worldwide trial locations. To find out more about past or current trials speak to your doctor and learn about the risks and potential benefits.
The MPS Society is the only UK charity at the forefront of supporting people and families affected by MPS and related diseases. Our extensive support services offer you a wide range of support and resources.
The team can advise and sign post you to adequate needs-led support and services in your local area as well as social care, home adaptions, education and much more.
The support team can visit you in your home and provide you with vital support.
Get involved and support us in the community, volunteer or support fundraising; we are a small charity but with your support we can continue to offer a highly valued and essential service.
Your stories

Story
When the unimaginable happens
As the world entered a new era, twenty years ago, of joy and optimism, for some life was taking them on a different course, to somewhere...
20/09/2022
Story
Dan's story - The Big Give Christmas Challenge 2021
Dan tells us why support services from the MPS Society are so important and how you can double your donation to fund them this Christmas.
15/11/2021
Story
Oliver and Sam
Oliver and Samuel are brothers and they both have MPS II Hunter disease because their bodies are missing a special enzyme.
01/12/2019
Latest news and blogs

News
Shining a light on the importance of individualised airway management plans
For Rare Disease Day, we shine the light on an important safety investigation report that involved insights from the MPS Society.
27/02/2024

Blog
Going on holiday in an MPS world
Living with MPS, Fabry or related condition can make going on holiday a daunting prospect. I am here to tell you that it's possible.
01/08/2023
Condition
Gene therapy clinical trial for patients with MPS II Hunter opens in Manchester
A new gene therapy clinical trial for patients with MPS II Hunter disease is opening in Manchester.
16/06/2023
Latest resources
Hunter Outcome Survey Patient Report 2023
Read the 2023 annual update of the Hunter Outcome Survey (HOS), a large disease registry which has facilitated the collection of data on the signs symptoms and progression of MPS II.
MPS II Hunter disease - information for individuals, parents and families
We know that being diagnosed with a rare disease is life-changing and you can struggle to come to terms with it. Therefore, we have...

Need someone to talk to?
Our support includes an active listening service and telephone helpline.